

Heart disease does not treat men and women the same way. The biology differs, the warning signs differ, and even the outcomes differ. Yet most people still picture a middle-aged man clutching his chest when they think about a heart attack.
That image leaves millions of women at risk. Cardiovascular disease remains the leading cause of death for women worldwide. The problem is not just the disease itself. It is how often it is missed, misunderstood, or treated too late.
Biology Tells a Different Story

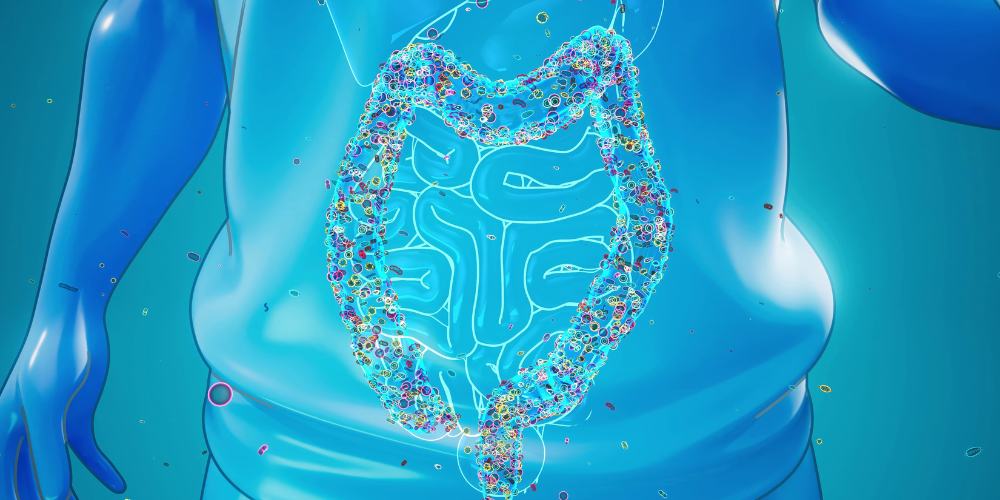
Puwadon / Pexels / Unlike women, men develop large blockages in the main coronary arteries. These blockages can rupture suddenly and cause a dramatic heart attack.
Doctors can usually spot these on standard angiograms because they create visible obstructions.
Women often face a different pattern. Many develop diffuse plaque spread throughout smaller vessels, along with microvascular dysfunction. That means blood flow is reduced even when major arteries appear clear. Conditions like INOCA and MINOCA are far more common in women, which makes diagnosis tricky and sometimes delayed.
Women also tend to have smaller coronary arteries. That difference alone can affect how procedures work and how symptoms show up. On top of that, women are more likely to experience spontaneous coronary artery dissection and stress-induced cardiomyopathy, also called Takotsubo syndrome.
Hormones shape much of this risk. Estrogen supports healthy blood vessels, improves cholesterol balance, and promotes nitric oxide production, which helps arteries relax. Before menopause, women have much lower rates of heart disease than men of the same age.
That advantage fades quickly after menopause. Within about ten years, women’s heart attack rates catch up to men’s. Blood pressure climbs, cholesterol shifts in the wrong direction, and body fat moves toward the abdomen. Insulin resistance increases, and the protective edge weakens.
Symptoms Often Get Brushed Off
Many women do not experience crushing chest pain during a heart attack. Instead, they report unusual fatigue, shortness of breath, nausea, jaw pain, or back discomfort. Some describe anxiety or a strange sense that something feels off.
For years, these symptoms were labeled atypical. That label caused real harm because it implied these signs were unusual or less serious. In reality, these symptoms are common in women. When doctors fail to recognize them as cardiac, the diagnosis gets delayed.
Women are more likely to be misdiagnosed during a heart attack. Some are sent home from emergency departments because their tests look normal at first glance. That delay can increase heart muscle damage and worsen long-term outcomes.
Risk factors also hit women differently. Diabetes increases heart disease risk in both sexes, but it raises the risk more sharply in women. Smoking also carries a stronger impact on younger women compared to men of the same age.
High blood pressure deserves special attention. Women often develop heart damage at lower blood pressure levels than men. Hypertension also increases the risk of heart failure and atrial fibrillation more strongly in women.
Pregnancy, Hormones, and Hidden Risk

Master / Pexels / Pregnancy can act like a stress test for the heart. Conditions such as preeclampsia, gestational diabetes, and preterm birth signal higher cardiovascular risk later in life.
These events are not just pregnancy complications. They are early warning signs.
Many women are never told that these pregnancy outcomes raise their long-term heart risk. Years pass, and the link gets forgotten. By the time symptoms appear in midlife, the opportunity for early prevention has slipped away.
Certain hormonal conditions also raise risk. Polycystic ovary syndrome is linked to insulin resistance and metabolic problems. Early menopause and premature ovarian insufficiency remove estrogen’s protective effects sooner than expected.
Autoimmune diseases add another layer. Conditions like lupus and rheumatoid arthritis are more common in women and increase inflammation throughout the body. Chronic inflammation accelerates atherosclerosis and raises cardiovascular risk.
Breast cancer treatment can also affect the heart. Some chemotherapy drugs and radiation therapies increase the risk of heart failure or coronary disease later on. Survivors may live for decades after treatment, but their heart risk remains elevated.